
Adrenal cancer occurs when cells in your adrenal glands mutate (change) and grow, forming a tumor.
Advanced Adrenal Cancer Treatment in Germany
An adrenal gland cancer is often associated with significant uncertainty. Whether the news follows weeks of unexplained hormonal symptoms, or is discovered as an incidental finding on a scan done for an entirely different reason, the questions that follow are immediate and urgent:
Patients commonly ask what the diagnosis means, how serious it is, and where they should seek specialized care Many patients and families seek care at international specialist centers that offer multidisciplinary oncology expertise that lead them to centers in Germany. Germany has a well-developed oncology system with specialized cancer centers and multidisciplinary tumour boards, and access to advanced treatment options for adrenal Cancer. Adrenal cancer treatment in Germany is typically includes surgical resection when possible, systemic therapies such as mitotane-based chemotherapy regimens, and radiotherapy in selected cases. In some clinical settings, patients may also have access to investigational therapies through clinical trials
Adrenal carcinoma, formally known as adrenocortical carcinoma (ACC), is a rare and aggressive malignancy. According to a comprehensive StatPearls review updated in 2025, the estimated annual incidence of ACC is 0.5 to 2 cases per million population, making it one of the rarest endocrine cancers globally [1]. It affects women more frequently than men, with a female predominance of 2.5:1 to 3:1, and most commonly presents in adults in their fourth to fifth decades of life [1].
Despite its rarity, adrenal gland malignancy is clinically significant because of its aggressive biology, frequent late-stage presentation, and limited effective systemic treatment options under standard care. When the diagnosis is confirmed and the urgency is real, clear clinical guidance and specialist evaluation are essential. TIG GmbH helps international patients understand what is genuinely possible in Germany about treatment options and access to specialized care. with a free initial case review and no pressure to commit.
What Is Adrenal Cancer?

Adrenal cancer is a malignancy originating in the adrenal glands, two small triangular organs that sit above the kidneys and produce vital hormones including cortisol, aldosterone, and androgens primarily in the adrenal cortex. Adrenocortical carcinoma (ACC) specifically arises from the outer cortex of the adrenal gland, the layer responsible for steroid hormone production. The tumour may be functioning, meaning it overproduces hormones and causes distinct clinical syndromes, or non-functioning, in which case it grows silently until it is large enough to press on surrounding structures.
Patients often ask what causes adrenal cancer. In most adults, ACC develops sporadically, without a clearly identified cause. However, research has identified associations with hereditary cancer syndromes, including Li-Fraumeni syndrome (often related to TP53 mutations), Lynch syndrome, and other germline genetic alterations [1]. A study of Danish ACC patients published in 2024 found an incidence rate of 1.4 per million per year and suggested a possible slight increase in incidence among women over time [2]. Functional hormone overproduction occurs in approximately 40–60% of cases, producing endocrine syndromes such as Cushing's syndrome or virilisation, while the remaining cases involve non-functional tumours detected incidentally or through mass-effect symptoms [1].
Symptoms and Diagnosis of Adrenal Cancer
One of the most challenging aspects of adrenal gland cancer is that its adrenal cancer symptoms are often subtle, non-specific, or easily attributed to other conditions, which is why many patients are diagnosed at an advanced stage. Studies show that 20–30% of adrenocortical carcinoma diagnoses are incidental findings, discovered during imaging done for an entirely unrelated reason [3].
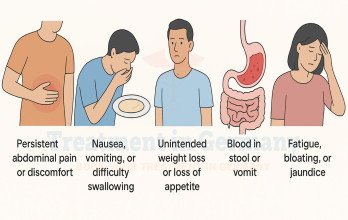
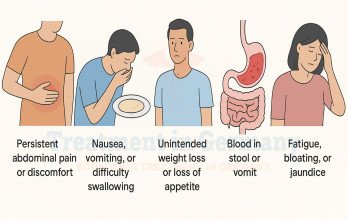
When symptoms do occur, they reflect either hormone overproduction or the physical growth of the tumour. Common adrenal gland cancer signs and symptoms include:
- Hormonal symptoms (functioning tumours): Cushing syndrome–like features such as central weight gain (face and abdomen), hypertension, muscle weakness, hyperglycemia, acne, and fatigue
- Adrenal gland tumor symptoms in females: in women, androgen excess may cause hirsutism (facial hair growth), voice deepening, menstrual irregularities, and virilisation, particularly in androgen-secreting tumor
- Mass-effect symptoms: abdominal or lower back pain, a palpable abdominal lump, unexplained weight loss, and poor appetite
- Metastatic adrenal cancer symptoms: in advanced or stage 4 adrenal cancer, bone pain, persistent fatigue or respiratory symptoms may suggest metastatic spread to distant organs
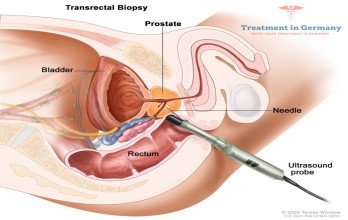
Diagnosis at specialist centers in Germany typically includes MRI, CT staging, hormonal evaluation, and PET-CT for suspected metastatic disease. In selected cases, particularly when metastatic disease or diagnostic uncertainty is present, tissue biopsy may be considered after exclusion of pheochromocytoma, Because adrenal carcinoma can be difficult to distinguish from a benign adenoma on imaging alone due to risk of catecholamine crisis, expert pathological and molecular analysis is essential, an area where German university hospitals have particular depth.
Types of Adrenal Cancer
Adrenal tumours are a heterogeneous group of diseases, and the tumor type strongly influences:
- Adrenocortical carcinoma (ACC): the most common and aggressive form of primary adrenal malignancy, arising from the hormone-producing outer cortex
- Pheochromocytoma: a tumour of the adrenal medulla is a neuroendocrine tumor of the adrenal medulla that may secrete excess catecholamines, leading to episodic or sustained hypertension, sweating, palpitations, and headaches
- Adrenal gland metastasis: cancer spreading to the adrenal gland from another organ such as the lung, breast, kidney, or colon; the most common cause of adrenal malignancy in adults overall

Adrenal Cancer Treatment in Germany: Available Treatment Options
Adrenal glands cancer treatment is rarely a single intervention. For the great majority of patients, it is a carefully coordinated sequence of therapies built around the specific tumour type, stage, and the patient's overall health. The major treatment modalities available through leading adrenal cancer clinics in Germany include surgery, chemotherapy, radiation therapy, and increasingly, interventional and immune-based approaches.

Adrenal Gland Surgery
Adrenal gland surgery, formally adrenalectomy, remains the cornerstone of curative-intent treatment for adrenal carcinoma. The primary surgical goal is complete removal of the tumour with clear margins (R0 resection). German centers performing adrenal tumour surgery offer:
- Laparoscopic adrenalectomy: minimally invasive approach used for smaller, localized adrenal tumors; however, in suspected or confirmed adrenocortical carcinoma, open surgery is often preferred due to risk of tumor capsule disruption and recurrence
- Open adrenalectomy: standard for larger or locally invasive tumours at Stage II–III to ensure complete margin clearance
- Cytoreductive surgery: used in selected Stage 4 adrenal cancer cases to reduce tumour burden before or alongside systemic therapy
- Resection of isolated metastases: pulmonary or hepatic metastasectomy in carefully selected patients who have responded to systemic treatment
Most patients can live well with a single functioning adrenal gland. Life expectancy with one adrenal gland is generally not compromised, provided the remaining gland is healthy and hormone levels are appropriately monitored. In cases requiring bilateral adrenalectomy, lifelong hormone replacement therapy is necessary.
Chemotherapy for Adrenal Cancer Treatment
Systemic chemotherapy is akey component of treatment for advanced or metastatic adrenocortical carcinoma, though options are limited and include chemotherapy and mitotane-based regimens. Mitotane (Lysodren) remains the only agent approved by both the US FDA and the European Medicines Agency specifically for adrenocortical carcinoma [4].The landmark FIRM-ACT trial, a randomised study involving 304 patients with advanced ACC, established that EDP-mitotane (etoposide, doxorubicin, cisplatin plus mitotane) demonstrated a higher response rate (~23%) and improved progression-free survival compared with streptozotocin plus mitotane in the FIRM-ACT trial, significantly outperforming the comparator arm [5]. This regimen remains the international standard for advanced adrenal gland cancer treatment.
German oncologists are experienced in managing mitotane toxicity, which requires careful therapeutic drug monitoring to maintain plasma levels within the effective therapeutic window. Studies have shown that maintaining therapeutic mitotane plasma concentrations is associated with improved outcomes in selected patients with adrenocortical carcinoma [6].
Radiation Therapy for Adrenal Cancer Treatment
Radiation is not a first-line treatment for most adrenal carcinomas, but it has a meaningful role in specific clinical situations:
- Adjuvant radiation may be considered in selected high-risk cases, but evidence for routine use is limited
- Stereotactic body radiation therapy (SBRT) may be used for palliation or local control of metastatic lesions (e.g., bone or lung), in selected cases
- Palliative radiation for pain control in end stage adrenal cancer, with high rates of symptom relief
Radiation may be used for local control or palliation in unresectable disease, but it is not considered curative in ACC
German centers delivering adrenal tumour treatment use the latest radiation platforms, including proton therapy and SBRT with sub-millimetre precision, allowing effective dose delivery while sparing surrounding healthy structures.
Immunotherapy for Adrenal Cancer in Germany
Adrenal cancer immunotherapy in Germany is one of the most actively evolving areas in the management of this disease. Checkpoint inhibitors, agents targeting PD-1, PD-L1, and CTLA-4, have been investigated in several clinical trials. A 2024 systematic review and meta-analysis published in Cancers found that immune checkpoint inhibitors demonstrated a modest overall efficacy but a good safety profile in advanced ACC, with some pooled analyses report median overall survival in the range of approximately 12–14 months in heavily pretreated patients [7]. Multiple clinical trials are ongoing, including studies of pembrolizumab, nivolumab combined with ipilimumab, and pembrolizumab with glucocorticoid receptor antagonists [8].
Innovative Adrenal Cancer Treatment Options in Germany
Beyond standard care, TIG GmbH supports international patients in accessing personalised cellular therapies within Germany's regulated clinical framework. The process includes treatment coordination, transparent cost structures, and practical travel support for international patients. Among these approaches, dendritic cell therapy is an investigational immune-based treatment being explored at selected specialist immunotherapy centres in Germany, although clinical evidence specific to adrenocortical carcinoma remains limited.
Dendritic Cell Therapy for Adrenal Cancer Treatment in Germany
Dendritic cell therapy (DCT), also called dendritic cell immunotherapy, is a personalised immune-based treatment designed to help the body recognise and respond to tumour-specific antigens. The concept originated from Ralph Steinman’s discovery of dendritic cells in 1973, a breakthrough that later earned him the Nobel Prize in Physiology or Medicine in 2011. In current clinical practice, the patient’s immune cells are collected and processed in a GMP-certified laboratory, where they are matured into active dendritic cells and exposed to tumour-associated antigens. These activated cells are then reinfused into the patient to stimulate a targeted cytotoxic immune response against cancer cells.

A 2023 peer-reviewed study in International Journal of Molecular Sciences described dendritic cells as an experimental immunotherapeutic approach being explored in multiple solid tumours, including rare endocrine cancers [9]. A 2025 review published in Cancers discussed the potential role of dendritic cell therapies in coordinating anti-tumour immune responses across multiple cancer settings, although disease-specific evidence in ACC remains limited [10].
Key features of dendritic cell therapy for adrenal cancer in Germany include:
- Built entirely from the patient's own immune cells, rejection risk is essentially absent
- Generally well tolerated alongside chemotherapy or radiation, with mild self-limiting side effects such as injection-site reactions and short-lived flu-like symptoms
- Suitable for adult patients with relapsed, refractory, or metastatic disease seeking an additional active option
- The potential for prolonged immune activity beyond treatment remains under investigation, though the duration and clinical impact of this effect remain under investigation
Outcomes vary between patients, and dendritic cell therapy for adrenal cancer is not a guaranteed cure. For selected patients with relapsed or advanced disease, dendritic cell therapy may be considered as part of a broader multimodal treatment strategy. To explore whether the current evidence supports this approach for your specific case, TIG GmbH can arrange a free specialist review.
TACE (Transarterial Chemoembolization) for Adrenal Cancer Treatment in Germany
TACE (Transarterial Chemoembolization) is a minimally invasive interventional oncology procedure in which chemotherapy is delivered directly into the arteries supplying the tumour, followed by targeted vascular embolization, starving the tumour of its blood supply while trapping the chemotherapy within it. In adrenal cancer, TACE is primarily used for liver tumors and selected hepatic metastases; its use in adrenocortical carcinoma is limited and not part of standard guideline-based care stage IV adrenocortical carcinoma where hepatic lesions are dominant or unresectable. The procedure may help reduce tumour burden, slow progression, and improve symptom control as part of a broader multimodal treatment strategy. TACE procedures in Germany are performed by experienced interventional radiologists under real-time imaging guidance.

The TACE treatment in Germany is particularly relevant for adrenal cancer in the following settings:
- Locally advanced or unresectable adrenal gland malignancy not amenable to surgical removal
- Stage 4 adrenal cancer with metastatic lesions that cannot be surgically addressed
- Tumour downsizing before planned surgery to improve resection margins
- Disease recurrence following prior surgery or systemic therapy
Transarterial chemoembolization is not considered curative, but is a recognised locoregional disease-control strategy used selectively in specialized centers. As a form of locoregional therapy within interventional oncology in Germany, TACE for adrenal cancer in Germany is offered at specialist centers with advanced radiology infrastructure, where it is frequently integrated into multimodal treatment plans alongside systemic therapy.
TACP (Transarterial Chemoperfusion) for Adrenal Cancer Treatment in Germany
TACP (Transarterial Chemoperfusion) delivers a high concentration of chemotherapy locally into the tumour's arterial supply, without the embolic (blocking) component used in TACE. This sustained local drug infusion preserves blood flow while achieving very high local drug concentrations, making transarterial chemoperfusion suitable in situations where full vascular occlusion carries a higher risk, or where a combined locoregional and systemic approach is planned.

TACP may be considered in selected clinical situations at centers with advanced interventional radiology expertise. The procedure is personalised based on the tumours vascular anatomy, location, and the patient's overall treatment objectives. It is often used alongside TACE or systemic therapy as part of a broader adrenal cancer treatment strategy.
Cost of Adrenal Cancer Treatment in Germany: TACE, TACP, and Dendritic Cell Therapy
The cost of TACE and TACP procedures as part of adrenal cancer treatment in Germany typically ranges between €8,000 and €9,000 per session, depending on the complexity of the case, imaging requirements, and number of treatments needed. These advanced interventional oncology therapies are performed by experienced specialists such as Thomas Vogl, internationally recognised for embolization therapies and locoregional cancer treatment.
The cost of dendritic cell therapy during adrenal cancer treatment in Germany is approximately €27,000 for total treatment course, although pricing may vary depending on the number of vaccine cycles and combined therapies used. Dendritic cell immunotherapy is delivered at specialised centres by experts such as Frank Gansauge at LDG Laboratories as part of personalised immune-based cancer treatment programmes.
Survival Rates and Prognosis
Adrenal cancer prognosis depends heavily on tumour stage at diagnosis, whether surgery achieved complete margins, hormonal secretion status, and access to specialist multidisciplinary care. Adrenal cancer survival rate should be interpreted carefully. Population-level data cannot predict an individual patient's outcome, and many factors influence how a specific patient will respond to treatment. Survival estimates vary significantly depending on tumour biology, hormonal activity, completeness of surgical resection, and access to specialist multidisciplinary care.
Table 1: Approximate estimates derived from published registry and outcomes data.

Overall 5-year survival for adrenal gland cancer across all stages is approximately 47–54%, though this varies significantly depending on stage and treatment received [11]. The 5-year survival rates for Stage I and Stage II ACC are approximately 80% and 60% respectively, while stage 4 adrenal cancer carries a 5-year survival rate of less than 15% among patients with metastatic disease [7].
Many patients and families ask about adrenal cancer stage 4 life expectancy. Stage 4 adrenocortical carcinoma remains a serious diagnosis with limited long-term survival that in chemotherapy trials has been reported around 14.8 months with EDP–mitotane [5]. However, access to multimodal treatment, including surgery, TACE, immunotherapy, and TACP, can meaningfully extend and improve survival in selected patients. How fast do adrenal tumours grow? ACC often demonstrates aggressive biological behaviour and rapid progression, which underlines the importance of reaching a specialist center without delay.
Best Hospitals for Adrenal Cancer Treatment
Through TIG GmbH, international patients access leading German hospitals with specialized endocrine oncology, interventional radiology, and adrenal tumour programmes:
Table 2: Leading Hospitals for Adrenal Cancer Treatment in Germany

Each centre operates within Germany's strict regulatory framework, runs dedicated tumour boards for rare endocrine malignancies, and participates in European research networks including ENSAT (European Network for the Study of Adrenal Tumors), giving patients access to the most current treatment standards and clinical trial opportunities.
Limitations and Considerations in Adrenal Cancer Treatment
Adrenal cancer treatment outcomes vary considerably depending on tumour stage, secretory status, surgical resection quality, and individual response to systemic therapy. Standard treatments including surgeryas the only potentially curative option for localized disease, while systemic therapy and radiotherapy are used mainly in advanced or selected cases. While Germany offers access to a broad range of advanced therapies, it is important that patients and families have realistic expectations: adrenal gland carcinoma prognosis in advanced stages remains challenging, and no treatment modality currently available, including cellular immunotherapy or interventional procedures, should be regarded as a guaranteed cure. Investigational approaches such as dendritic cell therapy are offered in a regulated, evidence-informed setting, and their suitability is always assessed individually by the treating specialist team. Treatment decisions are best made in specialist centres where multidisciplinary review ensures that the most appropriate and personalised plan is developed for each patient.
Why Choose Germany for Adrenal Cancer Treatment?
Patients from the United States, the United Kingdom, and across Europe choose Germany for adrenal gland cancer treatment because of its combination of clinical depth, strict regulatory standards, and coordinated specialist care. German oncology centers operate within a structured healthcare system where treatment decisions are guided by multidisciplinary review and evidence-based protocols. Many specialists contribute to international research on ACC and are active members of ENSAT, ensuring that patients treated in Germany benefit from the most current knowledge.
For patients considering where to pursue adrenal cancer treatment, Germany offers a well-established system of specialist hospitals, experienced multidisciplinary teams, and structured care pathways. Through TIG GmbH, international patients receive personalised treatment planning, transparent guidance, and coordinated support from initial review through to treatment and long-term follow-up.
How TIG GmbH Supports International Patients
TIG GmbH (Treatment in Germany) handles every step of the treatment in Germany journey:
- Free specialist review of your adrenal cancer diagnosis and treatment history
- Matching to the right oncology team based on stage, biology, and prior therapy
- Visa support and flight coordination
- On-site interpreter services and full medical report translation for your home oncologist
- Fixed-price billing with direct hospital payment
- Post-treatment coordination for 24 months after returning home
Begin your treatment journey today by submitting your reports through TIG GmbH (Treatment in Germany) and receiving a free, personalized response within 24 hours.
References
3. Cleveland Clinic. Adrenocortical Carcinoma: Symptoms, Stages & Prognosis.
9. Galati D, Zanotta S. Dendritic Cell and Cancer Therapy. Int J Mol Sci. 2023;24(4):4253. PMC9968100.
Why Patients Worldwide Prefer Our Medical Services in Germany – Key Benefits Explained
























.webp)
 (1).webp)
.webp)

.jpg)

 (1).webp)


.jpg)